Tilbudsguide, uge 45, 2019
And og æg!
Tilbudsguide, uge 44, 2019
Svinemørbrad og mandler!
Tilbudsguide, uge 43, 2019
Havregryn og oksefilet!
Tilbudsguide, uge 42, 2019
Olivenolie, granatæble og mango!
Vi har 65790 registrerede brugere. Nyeste registrede medlem er peinoin
Vores medlemmer har i alt skrevet 2049602 indlæg i 100423 emner
0 nye indlæg i dag



Changes in muscle morphology and neuromuscular function with eccentric strength training – consequences for athletic performance
Eccentric (ECC) muscle contractions denote situations in which active muscles generate contractile force while at the same time increasing their origin-to-insertion length. Conversely, concentric muscle contractions are characterized by a decrease in origin-to-insertion muscle length. In everyday life, eccentric muscle actions are mostly involved with the deceleration or damping of specific limb movements, for example in downhill running, when descending stairs or when landing from a jump. However, certain types of movements, especially within sports and exercise, involve maximal or nearmaximal eccentric muscle forces. One example is the take-off phase in maximal jumping.
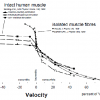
When recorded in isolated muscle preparations, ECC contraction force is substantially greater than that observed during concentric contraction (Fig.1). For the intact muscle in vivo, however, a marked suppression in maximal ECC contraction strength may be observed in untrained subjects (Figs.1, 3), suggesting that the pattern of neural motor outflow is of particular importance for the expression of maximal muscle strength during ECC contraction.

Fig.1 Force-velocity relationships obtained during concentric and eccentric contractions of isolated single muscle fibers, and during voluntary activation (triangles) and percutanous electrical muscle stimulation (open boxes) or when electrical stimulation was applied to ongoing maximal voluntary contraction (closed boxes) [reference 32].
Why is ECC muscle strength important?
High ECC muscle forces can be found in rapid stretch-shortening-cycle (SSC) movements, i.e. during maximal sprint running and jumping, alpine skiing, karate, weight lifting, etc. Also, high ECC forces may be generated by antagonist muscles during fast, forceful limb movements. In SSC movements, high eccentric strength of the agonist and antagonist muscles allows eccentric pre-stretch phases to be short lasting, thereby allowing an increase in movement frequency (cadence) which in turn results in an increased movement speed (e.g. in sprint running). In ballistic type of limb movements, high ECC strength of the antagonist muscles may allow for a short phase of limb deceleration at the end range of motion, in turn increasing the time available for limb acceleration thus causing maximal movement speed to increase [2]. Moreover, high levels of ECC antagonist muscle strength represent an elevated potential for muscular joint stabilization that protect ligaments and capsular joint structures [3].
Effects of strength training on maximal ECC muscle strength
Heavy-resistance strength training appears to evoke marked increases in maximal ECC muscle strength [4-8] (Fig.2). In contrast, strength training using low resistance does not seem to have any effect on ECC muscle strength [7,9]. Men and women may demonstrate similar increases in maximal ECC strength in response to strength raining. With more prolonged training, however, continued increases in ECC muscle strength were observed to occur only in male subjects [4], suggesting that the range of adaptation in ECC strength may differ between men and women. Regardless, strength training involving maximal eccentric or coupled eccentric-concentric muscle contractions generally appears to induce greater overall strength gains than concentric training alone, as indicated by data obtained both in male and female subjects [4,10,11].

Fig.2 Maximal concentric and eccentric quadriceps muscle strength measured as isokinetic peak moment (triangles) and angle-specific moment generated at 500 knee joint angle (boxes) (00 = full knee extension), before and after 12 wks of heavy-resistance strength training. Maximal eccentric and slow concentric muscle strength increased markedly following a period of heavy-resistance strength training (** P < 0.01, ** P < 0.05) [7].
Neuromuscular activation during maximal ECC contraction - effects of strength training
Neuromuscular activation appears to be reduced during maximal voluntary eccentric muscle contraction in untrained subjects, suggesting the presence of a neural inhibitory mechanism [8,12,13] (Fig.1). In result, the strength-speed relationship recorded for voluntarily activated human muscle does not resemble the force-velocity relationship obtained in isolated muscle very well (Fig.2). Notably, the inhibition in neuromuscular activation observed during ECC contraction appears to be reduced or fully removed in response to heavy-resistance strength training [8] (Fig.3). In addition, ECC strength training appears to induce large increases in EMG amplitude during ECC contraction, together with significant albeit less marked increases during concentric contraction [10,11].
Changes in muscle size and structure with ECC strength training
Maximal eccentric or coupled concentric-eccentric strength training appears to evoke greater increases in anatomical muscle cross-sectional area (CSA) obtained by MRI, CT or anthropometry measures, compared to concentric training alone [6,10,14] (Fig.4). Further, ECC strength training was reported to induce greater increases in muscle fiber CSA evaluated by biopsy sampling [11,15,16]. Interestingly, more long-lasting hypertrophy was observed during detraining from ECC strength training compared to concentric training [15].
A remarkably high degree of muscle fiber hypertrophy (52% increased mean fiber area) was reported to occur in response to 8 wks of high-volume ECC ergometry training [17], a training regime that does not resemble conventional strength training or maximal ECC strength training. The implications of these findings remain unsettled. Also, an increased number of sarcomeres in-series were found in rats trained by decline running which involved substantial ECC muscle loading, compared to rats performing concentric training in terms of uphill running [18]. Whether eccentric strength training can evoke a similar upregulation in fiber sarcomere number remains unknown. An increase in muscle fiber length would be highly beneficial, as this would result in an increased maximal shortening speed and hence elevated contractile power production.

Fig.3 Heavy-resistance strength training results in marked increases in maximal eccentric muscle strength (quadriceps muscle) (top panel). During maximal ECC contraction, characterized by high levels of contractile force generation, neuromuscular activation appears to be suppressed in untrained subjects (bottom panel). This inhibition in neuromuscular activation was removed partially (VL, VM) or fully (RF) after a period of strength training [8].
What are the physiological stimuli involved with ECC strength training?
Numerous candidates may be responsible for initiating the physiological adaptation processes associated with ECC strength training: high levels of contractile muscle force, disruption of the cytoskeleton, large muscle strains (i.e. loading at long fiber lengths), inflammatory responses, activation of satellite cells, as well as multi-factorial combinations of these factors.
In ECC contraction excessive muscle strain rather than large contractile forces appear to be detrimental to the cytoskeleton [19], causing desmin intermediate filaments to be disrupted [20] with a following loss of transversal fiber stability. This may render the muscle fibers vulnerable to further disruption of the cytoskeleton [20], in turn initiating inflammatory processes that may activate dormant satellite cells [21]. Upon activation a number of satellite cells would undergo fusion with the myofiber to provide additional nuclei to the interior of the muscle cell [22.23], thereby contributing to the elevated muscle protein synthesis observed with strength training. Also, excessive ECC muscle loading may induce sarcomere "popping" due to non-uniform sarcomere extension throughout the muscle fiber [24], thereby contributing to the process of myofibrillar disruption.

Fig.4 Changes in quadriceps muscle cross-sectional area (CSA) obtained by MRI before and after 10 wks of either concentric (CONC) or eccentric (ECC) strength training. Although quadriceps CSA increased in response to both CONC and ECC training (* P < 0.05), significantly greater changes occur with ECC training (**, arrows) [10].
Muscle protein turnover is influenced by growth factors produced locally within the muscle. Insulinlike growth factor I (IGF-I) increase in the muscle acutely following ECC strength training [25,26]. This rise in locally expressed IGF-I may facilitate myofiber hypertrophy by directly stimulating myofibrillar protein synthesis and/or inducing satellite cell growth, differentiation and fusion [26].
Use of eccentric strength training in overuse injury rehabilitation
ECC muscle-tendon loading regimes recently have demonstrated promising results in terms of injury rehabilitation. Thus, conditions such as Achilles tendinosis [27], anterior patella-femoral pain [28], patella tendon pain and jumpers knee [29] may show remarkable improvements following specially designed ECC training regimes. However, the specific mechanisms remain unknown.
ECC strength training in rats resulted in increased collagen turnover and a marked neoformation of vinculin and talin [30], which are key cytoskeletal proteins involved in the force transduction between muscle fibers and the myotendinous junction. Further, as demonstrated in rats a progressive neoformation of transversal collagen cross-links occurs at increasing age, causing tendons to become stiffer [31]. However, endurance training fully abolished this age related increase in collagen crosslink formation [31]. As a hypothesis, ECC strength training may be even more effective in doing so.
Eccentric strength training: practical implications
Maximal ECC strength training (i.e. loads > 1RM) should be performed only in individuals with several years of heavy-resistance training background. Importantly, correct lifting techniques should be employed at all time. Sufficient restitution time (5 days - 2 wks) should be allowed between training sessions, depending on the muscle groups trained, training status, and the number of sets performed. To facilitate the muscle hypertrophy response, timed protein intake (10-20 g) could be applied both prior to (20-60 min) as well as immediately after (0-10 min) ECC resistance exercise.
REFERENCES
- Westing et al., Acta Physiol. Scand. 140, 17-22, 1990
- Jaric et al., Eur. J. Appl. Physiol. 71, 464-468, 1995
- Aagaard et al., Am. J. Sports Med. 26, 231-237, 1998
- Colliander & Tesch, Acta Physiol. Scand. 141, 149-156, 1990
- Narici et al., Eur. J. Appl. Physiol. 59, 310-319, 1989
- Seger et al., Eur. J. Appl. Physiol. 79, 49-57, 1998
- Aagaard et al., Acta Physiol. Scand. 156, 123-129, 1996
- Aagaard et al., J. Appl. Physiol. 89, 2249-2257, 2000
- Duncan et al., J. Orthop. Sports Phys. Ther. 11, 70-75, 1989
- Higbie et al., J. Appl. Physiol. 81: 2173-81, 1996
- Hortobagyi et al., J. Appl. Physiol. 80, 765-772, 1996
- Westing et al., Eur. J. Appl. Physiol. 62, 104-108, 1991
- Amiridis et al., Eur. J. Appl. Physiol. 73, 149-56, 1996
- Walker et al., Arch. Phys. Med. Rehab. 79, 1391-1398, 1998
- Hather et al., Acta Physiol. Scand. 143, 177-185, 1991
- Hortobagyi et al., J. Physiol. 524, 293-304, 2000
- LaStayo et al., Am. J. Physiol. 278, R1282-1288, 2000
- Lynn & Morgan, J. Appl. Physiol. 77, 1439-1444, 1994
- Lieber & Friden, J. Appl. Physiol. 74, 520-526, 1993
- Lieber et al., J. Appl. Physiol. 80, 278-284, 1996
- Vierck et al., Cell Biol. Int. 24, 263-272, 2000
- Kadi et al., Med. Sci. Sports Exerc. 31, 1528-1534, 1999
- Kadi, Acta Physiol. Scand. Suppl. 646, 5-47, 2000
- Morgan & Allen, J. Appl. Physiol. 87, 2007-2015, 1999
- Yan et al., J. Appl. Physiol. 74, 410-414, 1993
- Bamman et al., Am. J. Physiol. 280, E383-390, 2001
- Alfredson et al., Am. J. Sports Med. 26, 360-366, 1998 1998
- Werner & Eriksson, Knee Surg. Sports Traumatol. Arthrosc. 1, 162-168, 1993
- Jonsson & Alfredson 2005, Br. J. Sports Med. 39, 847-850, 2005
- Frenette & Cote, Int. J. Sports Med. 21, 313-320, 1999
- Gosselin et al., J. Appl. Physiol. 85, 1011-1016, 1998
- Aagaard & Thorstensson, Chap. 1.4 in Textbook of Sports Medicine (Eds Kjær M et al), Blackwell, 2003